Download Cna Shower Sheets Template
Misconceptions
When it comes to the CNA Shower Sheets form, several misconceptions can lead to confusion. Understanding the facts can help improve the care provided to residents. Here are five common misconceptions:
- Misconception 1: The form is only for reporting severe skin issues.
- Misconception 2: The visual assessment is optional.
- Misconception 3: Only the charge nurse can fill out the form.
- Misconception 4: The form is only for skin conditions.
- Misconception 5: Once submitted, the form is no longer needed.
Many people believe that the CNA Shower Sheets form is only necessary for serious skin problems. In reality, it is essential for documenting even minor issues like dryness or scratches. Early detection can prevent more significant problems later on.
Some may think that performing a visual assessment of the resident's skin is optional. However, this assessment is a critical part of the showering process. It ensures that any abnormalities are noted and addressed promptly.
While the charge nurse plays a vital role in reviewing the form, CNAs are responsible for completing it during their shift. This documentation is crucial for effective communication within the care team.
Some individuals think the form solely focuses on skin conditions. However, it also includes a section for assessing toenail care, which is equally important for the resident’s overall health and comfort.
Another common belief is that the form is no longer relevant once it is submitted. In truth, the information collected should be continuously reviewed and monitored to ensure that any changes in the resident's condition are addressed promptly.
File Details
| Fact Name | Description |
|---|---|
| Purpose | The CNA Shower Sheets form is used for documenting skin assessments during resident showers. |
| Skin Monitoring | CNA staff must perform a visual assessment of the resident's skin while showering. |
| Reporting Abnormalities | Any abnormal skin findings must be reported to the charge nurse immediately. |
| Documentation | The form allows for specific documentation of the location and description of skin abnormalities. |
| Visual Assessment Criteria | The form includes a list of 15 skin conditions to monitor, such as bruising, rashes, and blisters. |
| Toenail Care | There is a section to indicate if the resident needs toenail trimming, with options for yes or no. |
| Signatures Required | The form requires signatures from both the CNA and the charge nurse to confirm assessments. |
| Forwarding Issues | Any problems identified must be forwarded to the Director of Nursing (DON) for further review. |
| Governing Law | This form is governed under Missouri state regulations related to resident care and nursing practices. |
Key takeaways
Filling out the CNA Shower Sheets form is an important task for ensuring the health and safety of residents. Here are key takeaways to keep in mind:
- Visual Assessment: Conduct a thorough visual assessment of the resident’s skin during the shower.
- Immediate Reporting: Report any abnormalities to the charge nurse right away.
- Documentation: Use the form to document the exact location and description of any skin abnormalities.
- Body Chart: Utilize the body chart included in the form to graphically represent skin issues by number.
- Skin Issues: Be aware of various skin conditions to monitor, including bruising, rashes, and lesions.
- Toenail Care: Determine if the resident needs toenail trimming and mark accordingly.
- Charge Nurse Signature: Ensure the charge nurse reviews and signs the form after assessment.
- Interventions: Document any interventions that are necessary based on the charge nurse's assessment.
- Forwarding Information: Indicate if the information has been forwarded to the Director of Nursing (DON).
- Confidentiality: Maintain the confidentiality of the resident's information throughout the process.
By following these guidelines, you can help ensure that residents receive the best possible care and that any issues are addressed promptly.
Dos and Don'ts
When filling out the CNA Shower Sheets form, it is essential to follow certain guidelines to ensure accuracy and compliance. Here are seven things you should and shouldn't do:
- Do perform a thorough visual assessment of the resident's skin during the shower.
- Do report any abnormal findings to the charge nurse immediately.
- Do accurately describe and graph all skin abnormalities on the body chart provided.
- Do ensure all required signatures are obtained, including yours and the charge nurse's.
- Don't leave any sections of the form blank; complete all fields as necessary.
- Don't use vague descriptions; be specific about the location and nature of any abnormalities.
- Don't forget to forward any issues to the Director of Nursing for further review.
Common mistakes
-
Failing to accurately document the resident's name and date at the top of the form. This information is crucial for tracking and reference.
-
Not performing a thorough visual assessment of the resident's skin. Skipping this step can lead to missed abnormalities that need attention.
-
Overlooking to report abnormalities to the charge nurse immediately. Timely reporting is essential for proper care.
-
Neglecting to use the body chart effectively. It's important to mark the exact location of any abnormalities for accurate communication.
-
Using vague descriptions for abnormalities instead of being specific. Clear descriptions help in understanding the severity of the issue.
-
Not indicating if the resident needs toenails cut. This is a simple yet important detail that can affect the resident's comfort and hygiene.
-
Forgetting to obtain the charge nurse's signature. This step is necessary to validate the assessment and intervention.
-
Failing to document the charge nurse's assessment and intervention. This information is vital for continuity of care.
-
Not forwarding the form to the Director of Nursing (DON) when required. This ensures that any serious issues are escalated appropriately.
What You Should Know About This Form
-
What is the purpose of the CNA Shower Sheets form?
The CNA Shower Sheets form is designed to help certified nursing assistants (CNAs) document a resident's skin condition during showers. It ensures that any abnormalities are noted and reported promptly to the charge nurse for further evaluation.
-
What should I do if I notice an abnormality on a resident's skin?
If you observe any abnormal skin conditions, such as bruising, rashes, or lesions, you must report these findings to the charge nurse immediately. Use the form to accurately describe the location and nature of the abnormality.
-
What types of skin conditions should be monitored?
The form includes a list of specific skin conditions to monitor, including:
- Bruising
- Skin tears
- Rashes
- Swelling
- Dryness
- Soft heels
- Lesions
- Decubitus ulcers
- Blisters
- Scratches
- Abnormal color
- Abnormal skin texture or temperature
- Other conditions as noted
-
How do I document the findings on the form?
Document your findings by using the body chart provided on the form. Assign numbers to each abnormality and describe them clearly. Ensure that your signature and date are included for accountability.
-
What happens after I submit the form?
Once you complete the form, it should be forwarded to the charge nurse for assessment. The charge nurse will review your findings and determine if further action is needed. The information may also be sent to the Director of Nursing (DON) if necessary.
-
Is there a section for toenail care on the form?
Yes, the form includes a question about whether the resident needs their toenails cut. This is an important aspect of overall skin and foot care, particularly for residents with mobility issues.
-
Who is responsible for signing off on the assessment?
The charge nurse is responsible for signing the form after reviewing the assessment. Additionally, the DON may also sign if the situation requires further intervention.
-
Where can I find more information about the CNA Shower Sheets form?
More information and access to the form can be found at www.primaris.org. This site provides resources related to quality improvement in healthcare.
-
What should I do if I have questions about using the form?
If you have questions regarding the use of the CNA Shower Sheets form, consult your supervisor or charge nurse. They can provide guidance and clarify any uncertainties about the documentation process.
Cna Shower Sheets Example
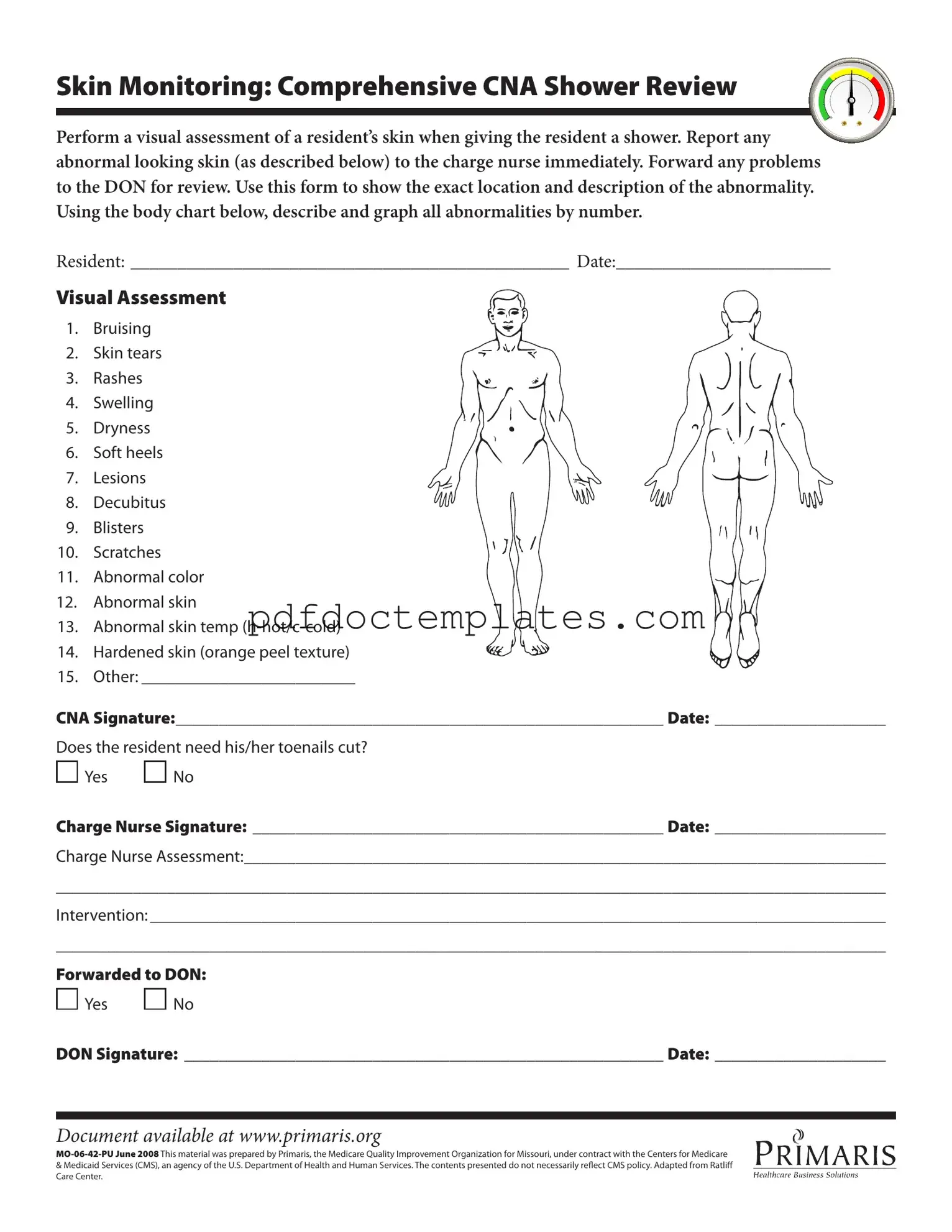
Skin Monitoring: Comprehensive CNA Shower Review
Perform a visual assessment of a resident’s skin when giving the resident a shower. Report any abnormal looking skin (as described below) to the charge nurse immediately. Forward any problems to the DON for review. Use this form to show the exact location and description of the abnormality. Using the body chart below, describe and graph all abnormalities by number.
RESIDENT: _______________________________________________ DATE:_______________________
Visual Assessment
1. Bruising
2. Skin tears
3. Rashes
4. Swelling
5. Dryness
6. Soft heels
7. Lesions
8. Decubitus
9. Blisters
10. Scratches
11. Abnormal color
12. Abnormal skin
13. Abnormal skin temp
14. Hardened skin (orange peel texture)
15. Other: _________________________
CNA Signature:_________________________________________________________ Date: ____________________
Does the resident need his/her toenails cut?

 Yes
Yes 
 No
No
Charge Nurse Signature: ________________________________________________ Date: ____________________
Charge Nurse Assessment:___________________________________________________________________________
_________________________________________________________________________________________________
Intervention: ______________________________________________________________________________________
_________________________________________________________________________________________________
Forwarded to DON:

 Yes
Yes 
 No
No
DON Signature: ________________________________________________________ Date: ____________________
Document available at www.primaris.org
&Medicaid Services (CMS), an agency of the U.S. Department of Health and Human Services. The contents presented do not necessarily relect CMS policy. Adapted from Ratlif Care Center.
Consider More Forms
How to Make a Character Sheet - An ambitious noble seeking to restore their family's lost honor.
For those looking to complete their transaction smoothly, the Arizona Trailer Bill of Sale form is crucial. This document facilitates the ownership transfer process, making it easier for the buyer to register their new trailer. To access this important form, click on the following link: necessary Arizona Trailer Bill of Sale paperwork.
Profits or Loss From Business - It captures all necessary data needed to compute the business’s income for tax purposes.