Download Acord 130 Template
Misconceptions
Understanding the Acord 130 form is crucial for businesses applying for workers' compensation insurance. However, several misconceptions can lead to confusion. Here are five common misunderstandings:
- The Acord 130 form is only for large businesses. Many people believe that only large companies need to complete this form. In reality, any business with employees, regardless of size, must fill out the Acord 130 to obtain workers' compensation coverage.
- Filling out the form is optional. Some individuals think that completing the Acord 130 is not mandatory. However, this form is essential for securing workers' compensation insurance, and failure to submit it can result in a denial of coverage.
- All information on the form is confidential. While many details on the Acord 130 are treated confidentially, some information may be shared with insurance companies or regulatory bodies. Understanding what can be disclosed is important for applicants.
- The Acord 130 form is the same in every state. Many assume that the Acord 130 is uniform across the United States. However, certain sections may vary depending on state regulations, so it’s important to check for state-specific requirements.
- Once submitted, the form cannot be changed. Some people think that once the Acord 130 is submitted, no changes can be made. In fact, if any information changes after submission, it is crucial to notify the insurance provider promptly to ensure that coverage remains valid.
Addressing these misconceptions can help ensure a smoother application process and better understanding of workers' compensation insurance requirements.
File Details
| Fact Name | Details |
|---|---|
| Purpose | The ACORD 130 form is used for applying for workers' compensation insurance, providing essential information about the applicant's business and its operations. |
| Governing Laws | Each state may have specific regulations governing workers' compensation. For instance, Missouri's regulations include requirements under Section 287.090 RSMo for exclusions. |
| Information Required | Applicants must provide comprehensive details, including business type, employee information, and prior insurance history, ensuring accurate risk assessment. |
| Submission Process | The form must be completed and submitted to an insurance agency. It can be bound or submitted as part of an assigned risk plan, depending on the applicant's situation. |
| Importance of Accuracy | Providing accurate information is crucial. Misrepresentation can lead to penalties, including fines or denial of coverage, as outlined in various state laws. |
Key takeaways
The Acord 130 form is essential for applying for workers' compensation insurance. Make sure to fill it out completely and accurately.
Include your agency information at the top of the form, including name, address, and contact details.
Clearly state your business details, such as the type of business entity (e.g., corporation, LLC) and years in operation.
Provide accurate employee information, including the number of full-time and part-time workers, as this affects your premium.
Be transparent about loss history for the past five years. This includes any claims made and their costs.
Check the exclusions section carefully. Certain employees or operations may need to be excluded from coverage.
Finally, ensure that the form is signed by an authorized representative of the business. This is crucial for the application to be valid.
Dos and Don'ts
When filling out the ACORD 130 form, it is crucial to approach the task with care and attention to detail. Here are four key dos and don'ts to keep in mind:
- Do double-check all entries for accuracy. Ensure that names, dates, and contact information are correct.
- Do provide complete information about your business operations. This helps underwriters assess your application accurately.
- Do include all required signatures. Missing signatures can delay the processing of your application.
- Do attach any necessary supporting documents, such as loss runs or additional remarks, to provide a clearer picture of your business.
- Don't leave any sections blank. If a question does not apply, indicate that clearly rather than omitting it.
- Don't provide false or misleading information. Misrepresentation can lead to severe penalties and denial of coverage.
- Don't rush through the form. Take your time to ensure that every detail is accurately represented.
- Don't forget to review your application before submission. A final review can catch errors that might have been overlooked.
Common mistakes
-
Incorrect Date Format: Failing to use the correct date format (MM/DD/YYYY) can lead to confusion and delays in processing your application.
-
Missing Agency Information: Not providing the agency name and address may result in your application being unprocessed or returned.
-
Incomplete Applicant Details: Omitting critical information, such as the applicant's name or contact details, can hinder communication and processing.
-
Incorrect Business Structure: Selecting the wrong type of business entity (e.g., corporation, LLC) can affect your coverage and liability.
-
Omitting Payroll Information: Not including accurate payroll figures for employees can lead to incorrect premium calculations.
-
Failure to List Exclusions: Neglecting to specify individuals who should be included or excluded from coverage may result in coverage gaps.
-
Inaccurate Loss History: Providing incorrect or incomplete loss history can affect your eligibility for coverage and premium rates.
-
Not Reviewing Responses: Failing to double-check all responses, especially to "Yes" or "No" questions, may lead to significant issues during underwriting.
What You Should Know About This Form
-
What is the Acord 130 form?
The Acord 130 form is a Workers Compensation Application used by businesses to apply for workers' compensation insurance. This form collects essential information about the applicant, including business details, employee classifications, and coverage needs.
-
Who needs to fill out the Acord 130 form?
Any business that employs workers and requires workers' compensation insurance must complete the Acord 130 form. This includes sole proprietors, corporations, partnerships, and other business entities.
-
What information is required on the Acord 130 form?
The form requires details such as the agency name, applicant's name, contact information, business structure, years in business, and estimated annual payroll. Additionally, applicants must provide information about their employees and any prior insurance history.
-
How do I determine my estimated annual premium?
Your estimated annual premium is calculated based on various factors, including the type of business, employee classifications, and payroll estimates. The form includes sections to help you outline these details, which will aid in determining the premium.
-
What are the different types of coverage available?
The Acord 130 form allows you to request various types of coverage, including workers' compensation, employer's liability, and any additional coverages or endorsements that may be necessary for your business operations.
-
What is the significance of the loss history section?
The loss history section is important because it provides the insurer with information about any past claims or losses your business has experienced. This history can impact your premium and the insurer's decision to provide coverage.
-
Are there any specific questions I should pay attention to?
Yes, the form includes questions that require detailed responses about your business operations, safety programs, and any past claims. These questions help assess the risk associated with insuring your business.
-
What happens if I provide false information on the form?
Providing false information can lead to serious consequences, including the denial of your insurance application, cancellation of coverage, or legal penalties. It is crucial to ensure that all information is accurate and truthful.
-
How do I submit the Acord 130 form?
You can submit the Acord 130 form through your insurance agent or broker. They will review the information and help you with the submission process to the appropriate insurance company.
-
Can I update the information on the Acord 130 form later?
Yes, if there are changes in your business operations or employee classifications, you should notify your insurer and update the information on the Acord 130 form. Keeping your information current is essential for maintaining appropriate coverage.
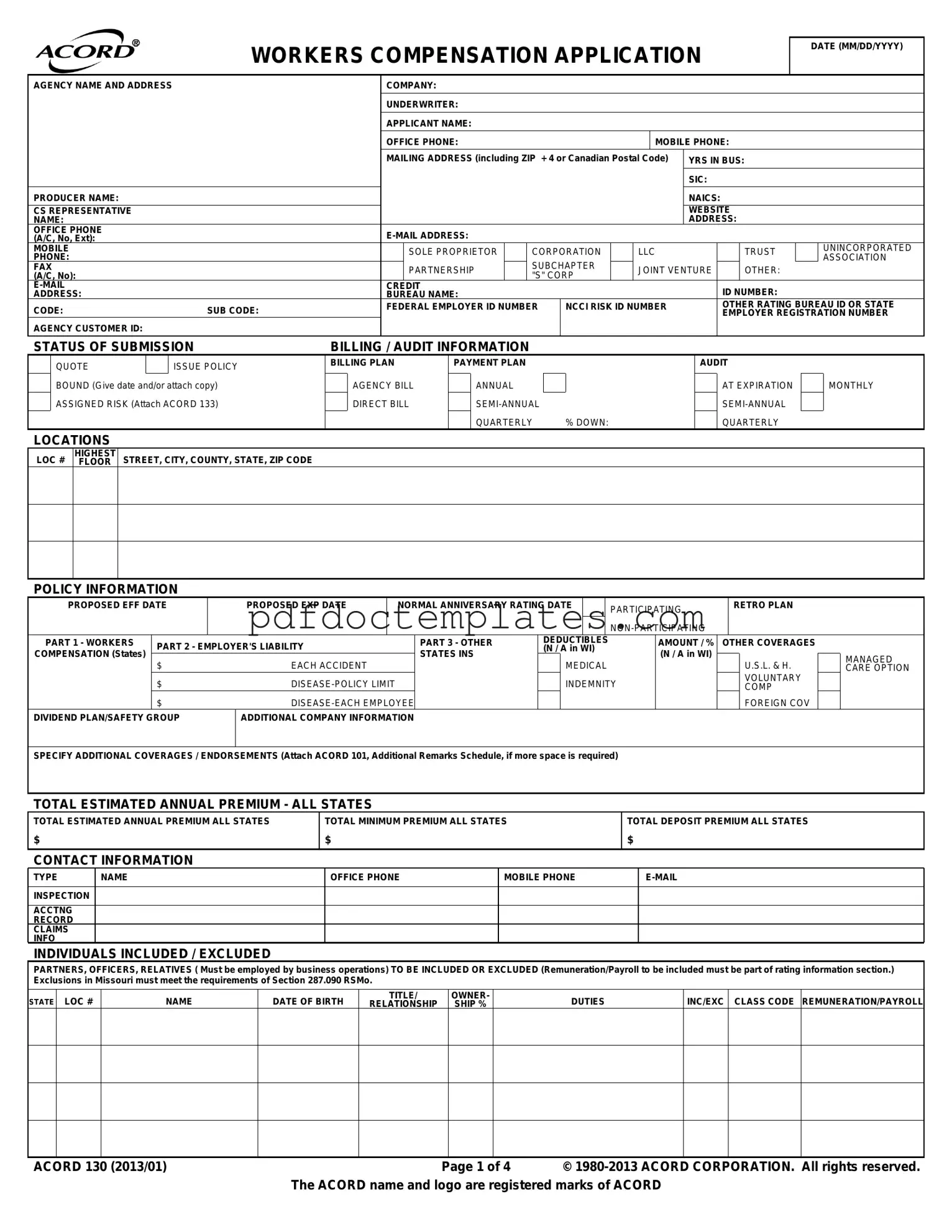
Acord 130 Example
WORKERS COMPENSATION APPLICATION |
DATE (MM/DD/YYYY) |
|
|
|
|
AGENCY NAME AND ADDRESS |
|
|
|
|
COMPANY: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
UNDERWRITER: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
APPLICANT NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
OFFICE PHONE: |
|
|
|
|
|
|
|
|
|
|
MOBILE PHONE: |
|
|
|
|||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
MAILING ADDRESS (including ZIP + 4 or Canadian Postal Code) |
YRS IN BUS: |
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SIC: |
|
|
|
|
|
|
|
|
||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
PRODUCER NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
NAICS: |
|
|
|
|
|
|
|
|
|||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
CS REPRESENTATIVE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
WEBSITE |
|
|
|
||||||||||||
NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ADDRESS: |
|
|
|
||||||||
OFFICE PHONE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
(A/C, No, Ext): |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
MOBILE |
|
|
|
|
|
|
|
|
|
|
|
|
|
SOLE PROPRIETOR |
|
|
CORPORATION |
|
LLC |
|
|
|
|
|
TRUST |
|
|
|
UNINCORPORATED |
||||||||||||||
PHONE: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ASSOCIATION |
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SUBCHAPTER |
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
FAX |
|
|
|
|
|
|
|
|
|
|
|
|
|
PARTNERSHIP |
|
|
|
JOINT VENTURE |
|
|
|
OTHER: |
|
|
|
||||||||||||||||||
(A/C, No): |
|
|
|
|
|
|
|
|
|
|
|
|
|
"S" CORP |
|
|
|
|
|
|
|
||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
CREDIT |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ID NUMBER: |
|
|
|
|||||||||||||
ADDRESS: |
|
|
|
|
|
|
|
|
|
|
BUREAU NAME: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||
CODE: |
|
|
|
|
|
|
SUB CODE: |
|
|
FEDERAL EMPLOYER ID NUMBER |
|
|
NCCI RISK ID NUMBER |
|
|
|
OTHER RATING BUREAU ID OR STATE |
||||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
EMPLOYER REGISTRATION NUMBER |
|||||||||||||
AGENCY CUSTOMER ID: |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||
STATUS OF SUBMISSION |
|
BILLING / AUDIT INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||
|
QUOTE |
|
|
|
ISSUE POLICY |
|
BILLING PLAN |
|
PAYMENT PLAN |
|
|
|
|
|
|
|
|
|
|
|
|
AUDIT |
|
|
|
||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||
|
BOUND (Give date and/or attach copy) |
|
|
AGENCY BILL |
|
|
ANNUAL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
AT EXPIRATION |
|
|
MONTHLY |
||||||||||||||||||
|
ASSIGNED RISK (Attach ACORD 133) |
|
|
DIRECT BILL |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
QUARTERLY |
|
|
% DOWN: |
|
|
|
|
|
|
|
QUARTERLY |
|
|
|
||||||||||
LOCATIONS |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||
LOC # |
HIGHEST |
|
STREET, CITY, COUNTY, STATE, ZIP CODE |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||
FLOOR |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
POLICY INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||||
|
PROPOSED EFF DATE |
|
|
PROPOSED EXP DATE |
|
|
NORMAL ANNIVERSARY RATING DATE |
|
|
PARTICIPATING |
|
|
|
|
RETRO PLAN |
|
|
|
|||||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|||||||
PART 1 - WORKERS |
PART 2 - EMPLOYER'S LIABILITY |
|
|
|
|
|
PART 3 - OTHER |
|
|
DEDUCTIBLES |
|
|
|
|
AMOUNT / % |
OTHER COVERAGES |
|
|
|
||||||||||||||||||||||||
|
|
|
|
|
|
|
(N / A in WI) |
|
|
|
|
|
|
||||||||||||||||||||||||||||||
COMPENSATION (States) |
|
|
|
|
|
STATES INS |
|
|
|
|
|
(N / A in WI) |
|
|
|
|
|
|
|
|
|
||||||||||||||||||||||
$ |
|
|
|
EACH ACCIDENT |
|
|
|
|
|
MEDICAL |
|
|
|
|
|
|
U.S.L. & H. |
|
|
MANAGED |
|||||||||||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
CARE OPTION |
|||||||||||||
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
INDEMNITY |
|
|
|
|
|
|
|
|
VOLUNTARY |
|
|
|
|||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
COMP |
|
|
|
|||||||||||||
|
|
|
|
|
|
$ |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
FOREIGN COV |
|
|
|
||||||||
DIVIDEND PLAN/SAFETY GROUP |
|
ADDITIONAL COMPANY INFORMATION |
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
||||||||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
SPECIFY ADDITIONAL COVERAGES / ENDORSEMENTS (Attach ACORD 101, Additional Remarks Schedule, if more space is required)
TOTAL ESTIMATED ANNUAL PREMIUM - ALL STATES
TOTAL ESTIMATED ANNUAL PREMIUM ALL STATES |
TOTAL MINIMUM PREMIUM ALL STATES |
TOTAL DEPOSIT PREMIUM ALL STATES |
$ |
$ |
$ |
|
|
|
CONTACT INFORMATION
TYPE |
NAME |
OFFICE PHONE |
MOBILE PHONE |
|
|
|
|
|
|
INSPECTION |
|
|
|
|
|
|
|
|
|
ACCTNG |
|
|
|
|
RECORD |
|
|
|
|
CLAIMS |
|
|
|
|
INFO |
|
|
|
|
INDIVIDUALS INCLUDED / EXCLUDED
PARTNERS, OFFICERS, RELATIVES ( Must be employed by business operations) TO BE INCLUDED OR EXCLUDED (Remuneration/Payroll to be included must be part of rating information section.) Exclusions in Missouri must meet the requirements of Section 287.090 RSMo.
STATE |
LOC # |
NAME |
DATE OF BIRTH |
TITLE/ |
OWNER- |
DUTIES |
INC/EXC |
CLASS CODE |
REMUNERATION/PAYROLL |
RELATIONSHIP |
SHIP % |
||||||||
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
|
ACORD 130 (2013/01) |
Page 1 of 4 |
© |
|
The ACORD name and logo are registered marks of ACORD |
|
STATE RATING SHEET # |
|
OF |
|
SHEETS |
AGENCY CUSTOMER ID: |
STATE RATING WORKSHEET
FOR MULTIPLE STATES, ATTACH AN ADDITIONAL PAGE 2 OF THIS FORM RATING INFORMATION - STATE:
LOC # CLASS CODE
DESCR
CODE
CATEGORIES, DUTIES, CLASSIFICATIONS
# EMPLOYEES
FULL PART
TIME TIME
SIC
NAICS
ESTIMATED ANNUAL
REMUNERATION/
PAYROLL
ESTIMATED
RATE ANNUAL MANUAL PREMIUM
PREMIUM
STATE: |
FACTOR |
FACTORED PREMIUM |
|
FACTOR |
FACTORED PREMIUM |
TOTAL |
N / A |
$ |
|
|
$ |
INCREASED LIMITS |
|
$ |
SCHEDULE RATING * |
|
$ |
DEDUCTIBLE * |
|
$ |
CCPAP |
|
$ |
|
|
$ |
STANDARD PREMIUM |
|
$ |
EXPERIENCE OR MERIT |
|
$ |
PREMIUM DISCOUNT |
|
$ |
MODIFICATION |
|
|
|||
|
|
$ |
EXPENSE CONSTANT |
N / A |
$ |
ASSIGNED RISK SURCHARGE * |
|
$ |
TAXES / ASSESSMENTS * |
N / A |
$ |
ARAP * |
|
$ |
|
|
$ |
* N / A in Wisconsin |
|
|
|
|
|
TOTAL ESTIMATED ANNUAL PREMIUM
$
MINIMUM PREMIUM
$
DEPOSIT PREMIUM
$
REMARKS (ACORD 101, Additional Remarks Schedule, may be attached if more space is required)
|
|
ACORD 130 (2013/01) |
Page 2 of 4 |
PRIOR CARRIER INFORMATION / LOSS HISTORY
AGENCY CUSTOMER ID:
PROVIDE INFORMATION FOR THE PAST 5 YEARS AND USE THE REMARKS SECTION FOR LOSS DETAILS |
|
|
|
LOSS RUN ATTACHED |
|
||
YEAR |
CARRIER & POLICY NUMBER |
ANNUAL PREMIUM |
MOD |
# CLAIMS |
AMOUNT PAID |
RESERVE |
|
|
CO: |
|
|
|
|
|
|
|
POL #: |
|
|
|
|
|
|
|
CO: |
|
|
|
|
|
|
|
POL #: |
|
|
|
|
|
|
|
CO: |
|
|
|
|
|
|
|
POL #: |
|
|
|
|
|
|
|
CO: |
|
|
|
|
|
|
|
POL #: |
|
|
|
|
|
|
|
CO: |
|
|
|
|
|
|
POL #:
NATURE OF BUSINESS / DESCRIPTION OF OPERATIONS
GIVE COMMENTS AND DESCRIPTIONS OF BUSINESS, OPERATIONS AND PRODUCTS: MANUFACTURING - RAW MATERIALS, PROCESSES, PRODUCT, EQUIPMENT; CONTRACTOR - TYPE OF WORK,
GENERAL INFORMATION
EXPLAIN ALL "YES" RESPONSES
1.DOES APPLICANT OWN, OPERATE OR LEASE AIRCRAFT / WATERCRAFT?
2.DO / HAVE PAST, PRESENT OR DISCONTINUED OPERATIONS INVOLVE(D) STORING, TREATING, DISCHARGING, APPLYING, DISPOSING, OR TRANSPORTING OF HAZARDOUS MATERIAL? (e.g. landfills, wastes, fuel tanks, etc)
3.ANY WORK PERFORMED UNDERGROUND OR ABOVE 15 FEET?
4.ANY WORK PERFORMED ON BARGES, VESSELS, DOCKS, BRIDGE OVER WATER?
5.IS APPLICANT ENGAGED IN ANY OTHER TYPE OF BUSINESS?
6.ARE
7.ANY WORK SUBLET WITHOUT CERTIFICATES OF INSURANCE? (If "YES", payroll for this work must be included in the State Rating Worksheet on Page 2)
8.IS A WRITTEN SAFETY PROGRAM IN OPERATION?
9.ANY GROUP TRANSPORTATION PROVIDED?
10.ANY EMPLOYEES UNDER 16 OR OVER 60 YEARS OF AGE?
11.ANY SEASONAL EMPLOYEES?
12.IS THERE ANY VOLUNTEER OR DONATED LABOR? (If "YES", please specify)
13.ANY EMPLOYEES WITH PHYSICAL HANDICAPS?
14.DO EMPLOYEES TRAVEL OUT OF STATE? (If "YES", indicate state(s) of travel and frequency)
15.ARE ATHLETIC TEAMS SPONSORED?
Y / N
ACORD 130 (2013/01) |
Page 3 of 4 |
GENERAL INFORMATION (continued)
AGENCY CUSTOMER ID:
EXPLAIN ALL "YES" RESPONSES
16.ARE PHYSICALS REQUIRED AFTER OFFERS OF EMPLOYMENT ARE MADE?
17.ANY OTHER INSURANCE WITH THIS INSURER?
18.ANY PRIOR COVERAGE DECLINED / CANCELLED /
19.ARE EMPLOYEE HEALTH PLANS PROVIDED?
20.DO ANY EMPLOYEES PERFORM WORK FOR OTHER BUSINESSES OR SUBSIDIARIES?
21.DO YOU LEASE EMPLOYEES TO OR FROM OTHER EMPLOYERS?
22.DO ANY EMPLOYEES PREDOMINANTLY WORK AT HOME? If "YES", # of Employees:
23.ANY TAX LIENS OR BANKRUPTCY WITHIN THE LAST FIVE (5) YEARS? (If "YES", please specify)
24.ANY UNDISPUTED AND UNPAID WORKERS COMPENSATION PREMIUM DUE FROM YOU OR ANY COMMONLY MANAGED OR OWNED ENTERPRISES? IF YES, EXPLAIN INCLUDING ENTITY NAME(S) AND POLICY NUMBER(S).
Y / N
SIGNATURE
Copy of the Notice of Information Practices (Privacy) has been given to the applicant. (Not required in all states, contact your agent or broker for your state's requirements.)
PERSONAL INFORMATION ABOUT YOU, INCLUDING INFORMATION FROM A CREDIT OR OTHER INVESTIGATIVE REPORT, MAY BE COLLECTED FROM PERSONS OTHER THAN YOU IN CONNECTION WITH THIS APPLICATION FOR INSURANCE AND SUBSEQUENT AMENDMENTS AND RENEWALS. SUCH INFORMATION AS WELL AS OTHER PERSONAL AND PRIVILEGED INFORMATION COLLECTED BY US OR OUR AGENTS MAY IN CERTAIN CIRCUMSTANCES BE DISCLOSED TO THIRD PARTIES WITHOUT YOUR AUTHORIZATION. CREDIT SCORING INFORMATION MAY BE USED TO HELP DETERMINE EITHER YOUR ELIGIBILITY FOR INSURANCE OR THE PREMIUM YOU WILL BE CHARGED. WE MAY USE A THIRD PARTY IN CONNECTION WITH THE DEVELOPMENT OF YOUR SCORE. YOU MAY HAVE THE RIGHT TO REVIEW YOUR PERSONAL INFORMATION IN OUR FILES AND REQUEST CORRECTION OF ANY INACCURACIES. YOU MAY ALSO HAVE THE RIGHT TO REQUEST IN WRITING THAT WE CONSIDER EXTRAORDINARY LIFE CIRCUMSTANCES IN CONNECTION WITH THE DEVELOPMENT OF YOUR CREDIT SCORE. THESE RIGHTS MAY BE LIMITED IN SOME STATES. PLEASE CONTACT YOUR AGENT OR BROKER TO LEARN HOW THESE RIGHTS MAY APPLY IN YOUR STATE OR FOR INSTRUCTIONS ON HOW TO SUBMIT A REQUEST TO US FOR A MORE DETAILED DESCRIPTION OF YOUR RIGHTS AND OUR PRACTICES REGARDING PERSONAL INFORMATION.
(Not applicable in AZ, CA, DE, KS, MA, MN, ND, NY, OR, VA, or WV. Specific ACORD 38s are available for applicants in these states.)
Any person who knowingly and with intent to defraud any insurance company or other person files an application for insurance containing any materially false information or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act, which is a crime and subjects that person to criminal and civil penalties (In Oregon, the aforementioned actions may constitute a fraudulent insurance act which may be a crime and may subject the person to penalties). (In New York, the civil penalty is not to exceed five thousand dollars ($5,000) and the stated value of the claim for each such violation). (Not applicable in AL, AR, AZ, CO, DC, FL, KS, LA, ME, MD, MN, NM, OK, PR, RI, TN, VA, VT, WA and WV).
Applicable in AL, AR, AZ, DC, LA, MD, NM, RI and WV: Any person who knowingly (or willfully in MD) presents a false or fraudulent claim for payment of a loss or benefit or who knowingly (or willfully in MD) presents false information in an application for insurance is guilty of a crime and may be subject to fines or confinement in prison.
Applicable in Colorado: It is unlawful to knowingly provide false, incomplete, or misleading facts or information to an insurance company for the purpose of defrauding or attempting to defraud the company, Penalties may include imprisonment, fines, denial of insurance and civil damages. Any insurance company or agent of an insurance company who knowingly provides false, incomplete, or misleading facts or information to a policyholder or claimant for the purpose of defrauding or attempting to defraud the policyholder or claimant with regard to a settlement or award payable from insurance proceeds shall be reported to the Colorado Division of Insurance within the department of regulatory agencies.
Applicable in Florida and Oklahoma: Any person who knowingly and with intent to injure, defraud, or deceive any insurer files a statement of claim or an application containing any false, incomplete, or misleading information is guilty of a felony (In FL, a person is guilty of a felony of the third degree).
Applicable in Kansas: Any person who, knowingly and with intent to defraud, presents, causes to be presented or prepares with knowledge or belief that it will be presented to or by an insurer, purported insurer, broker or any agent thereof, any written statement as part of, or in support of, an application for the issuance of, or the rating of an insurance policy for personal or commercial insurance, or a claim for payment or other benefit pursuant to an insurance policy for commercial or personal insurance which such person knows to contain materially false information concerning any fact material thereto; or conceals, for the purpose of misleading, information concerning any fact material thereto commits a fraudulent insurance act.
Applicable in Maine, Tennessee, Virginia and Washington: It is a crime to knowingly provide false, incomplete or misleading information to an insurance company for the purpose of defrauding the company. Penalties may include imprisonment, fines or a denial of insurance benefits.
Applicable in Puerto Rico: Any person who knowingly and with the intention of defrauding presents false information in an insurance application, or presents, helps, or causes the presentation of a fraudulent claim for the payment of a loss or any other benefit, or presents more than one claim for the same damage or loss, shall incur a felony and, upon conviction, shall be sanctioned for each violation by a fine of not less than five thousand dollars ($5,000) and not more than ten thousand dollars ($10,000), or a fixed term of imprisonment for three (3) years, or both penalties. Should aggravating circumstances be present, the penalty thus established may be increased to a maximum of five (5) years, if extenuating circumstances are present, it may be reduced to a minimum of two (2) years.
Applicable in Utah: Any person who knowingly presents false or fraudulent underwriting information, files or causes to be filed a false or fraudulent claim for disability compensation or medical benefits, or submits a false or fraudulent report or billing for health care fees or other professional services is guilty of a crime and may be subject to fines and confinement in state prison.
THE UNDERSIGNED IS AN AUTHORIZED REPRESENTATIVE OF THE APPLICANT AND REPRESENTS THAT REASONABLE INQUIRY HAS BEEN MADE TO OBTAIN THE ANSWERS TO QUESTIONS ON THIS APPLICATION. HE/SHE REPRESENTS THAT THE ANSWERS ARE TRUE, CORRECT AND COMPLETE TO THE BEST OF HIS/HER KNOWLEDGE.
APPLICANT'S SIGNATURE (Must be Officer, Owner or Partner)
DATE
PRODUCER'S SIGNATURE
NATIONAL PRODUCER NUMBER
ACORD 130 (2013/01) |
Page 4 of 4 |
Consider More Forms
Assurion Insurance - The F-017-08 MEN form is easy to fill out for convenience.
Bpo Template - The form will note whether the property has been previously listed on the market.
The importance of the Florida Operating Agreement form cannot be overstated, as it not only delineates the governance and operational framework of an LLC but also provides a basis for member relations. By clearly defining rights and responsibilities, this agreement helps to mitigate potential conflicts and misunderstandings. For those looking to create or amend their own agreements, resources like All Florida Forms are invaluable in ensuring compliance and clarity.
Workmanship Warranty Example - The certificate serves as an official recognition of the warranty issued by MCS Roofing.